您当前的位置:检测资讯 > 科研开发
嘉峪检测网 2022-07-14 22:10
聚 (ε-己内酯) (PCL) 作为性能良好的聚合物受到了广泛关注。本研究发现非炎性壳聚糖涂层促进软骨浸润到PCL支架内及其上方,并且与骨小梁整合兼容。体外成骨试验预测骨整合到多孔支架中的能力有限,因为在体内,编织骨从再生骨小梁的前缘整合,而不是从粘附在支架表面的间充质细胞整合,并且生物活性涂层吸引炎症细胞而诱导骨吸收。
01、研究内容简介
骨组织工程(BTE)策略旨在控制聚合物结构和生物活性,以促进骨生长成多孔支架。尽管在结构设计方面取得了很大进展,但在理解如何引导骨髓细胞和血管向内迁移和分化,以在多孔支架深处形成矿化组织方面仍然存在挑战。PCL作为首选的生物相容性聚合物受到了广泛关注,部分原因是生物塑料可以熔化形成不同的形状,支持间充质干细胞 (MSCs) 在体外的细胞浸润和成骨,并允许体内编织骨沉积(在外源细胞或生物活性因子的帮助下)。孔径是影响体内骨整合到不同材料中的一个重要因素。孔径≤100μm的支架显示出有限的血管化,同时促进软骨形成。血管化的骨会自发地渗入具有>100μm-850μm 孔的支架中,但通常仅限于外孔。
此前的研究开发了具有完全互连孔和精确孔径的 PCL 支架,以评估其潜力在 BTE 应用中。PCL 具有抑制细胞附着的疏水表面,这是体外成骨所必需的。因此,制定了一种用亲水性阳离子材料涂覆 PCL 支架孔表面的方法。这是通过聚电解质(PDADMAC作为聚阳离子和PSS 作为聚阴离子)的逐层自组装实现的。当 PCL 支架涂有 99% 脱乙酰度 (DDA) 壳聚糖时,骨髓间充质干细胞 (MSCs) 渗入 PCL 孔,在 3D体外成骨试验中产生更多矿化基质。基于这些有希望的结果,本研究的目的是使用已建立的骨骼成熟的兔骨软骨修复模型,评估99% DDA 壳聚糖涂层对 PCL 支架体内成骨的影响。
在这项研究中,作者认为血肿是植入后第一个占据 BTE 支架的组织。最近的数据表明,结构不同的壳聚糖具有不同的先天免疫激活潜力,可用于指导骨折修复反应。99% DDA 壳聚糖微粒在体外可在人巨噬细胞中诱导抗炎反应,包括释放干扰素 α 和白细胞介素 1 受体拮抗剂。因此,作者使用 99% DDA 10 kDa 壳聚糖来涂覆 PCL 支架,因为它具有细胞粘附性、非炎症性和体内潜在的抗炎活性。相比之下,约 80% DDA 壳聚糖微粒(但不大于 95%DDA)在掺入血肿时会特异性吸引中性粒细胞和巨噬细胞并刺激血管生成。因此作者通过将 不同的PCL 支架压入骨骺微钻缺损中以验证以下假设:当涂有 99% DDA 壳聚糖时,具有完全连通孔的 PCL 支架在体内骨整合更多,而当涂有 99% DDA壳聚糖+83% DDA壳聚糖微粒时,血管生成和成骨更多。仅钻孔缺陷作为自发修复的对照并在手术后 6 周分析了每种情况下 6 个骨软骨缺损的初始缺损和修复组织。
多孔 PCL 和壳聚糖涂层的制备:淬火后的45 vol% PCL/55 vol% PEO混合物分别退火1.5、2.0和2.5小时制造具有完全互连孔的 PCL 支架圆柱体,其中2 小时退火周期获得的155μm±8μm 孔径符合目标(图 1a 和 b)。直径3毫米,厚2毫米的PCL 圆柱体用交替的聚电解质逐层处理,然后用99%DDA壳聚糖与结构匹配的壳聚糖荧光示踪剂相结合(99PCL)。所有 99-PCL 支架表面均涂有 99% DDA 壳聚糖(约 1-3μm 厚的涂层,图 1c)。将不含荧光示踪剂 99-PCL 支架浸泡在含有 83% DDA RITC-壳聚糖示踪剂(83-99-PCL)的稀释 83% DDA 壳聚糖中,在 99PCL支架表面上获得了均匀的 83% DDA 壳聚糖表面涂层(图 1d)。可溶性 83% DDA 壳聚糖留在 83-99-PCL 孔隙空间中,以生产壳聚糖微粒。
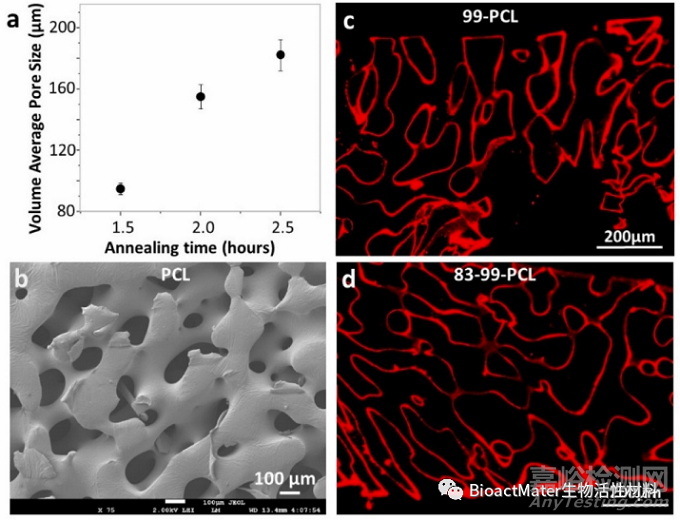
Fig. 1. Fabrication of porous PCL and chitosan coatings. (a) Scaffold blends of 45% PCL/55% PEO annealed for 1.5, 2 or 2.5 h yielded average pore sizes of 95 ± 4μm, 155 ± 8μm and 182 ± 10μm, respectively. (b) SEM image at 75× magnification of a PCL scaffold with average 155 μm pore diameter. Epifluorescent images of (c) 99-PCL (with RITC-99% DDA chitosan tracer) and (d) 8399-PCL (coated with unlabeled 99% DDA chitosan and then 83% DDA chitosan containing RITC83% DDA chitosan tracer).
“不对称”凝块趋化性测定:
分析先天免疫细胞 - 支架相互作用(图2)。在 37°C 的 1 小时内,外周血凝块细胞“蜂拥”到 83-99-PCL 支架上,与 99PCL 和 PCL 相比,支架周边的细胞密度高出2倍(p < 0.05,图2a-c),83-99-PCL凝块收缩却与另外3组凝块收缩相似(图2d)。如图2e和2f所示,凝块细胞可以吞噬部分99% DDA 壳聚糖涂层。至于 83% DDA 壳聚糖微粒,接近支架时越来越多地被吞噬细胞清除,最强烈的红色荧光细胞占据孔隙并沿着 83-99-PCL 支架周边聚集(图2g),即在体外血肿中对 83-99-PCL有选择性促炎趋化反应。
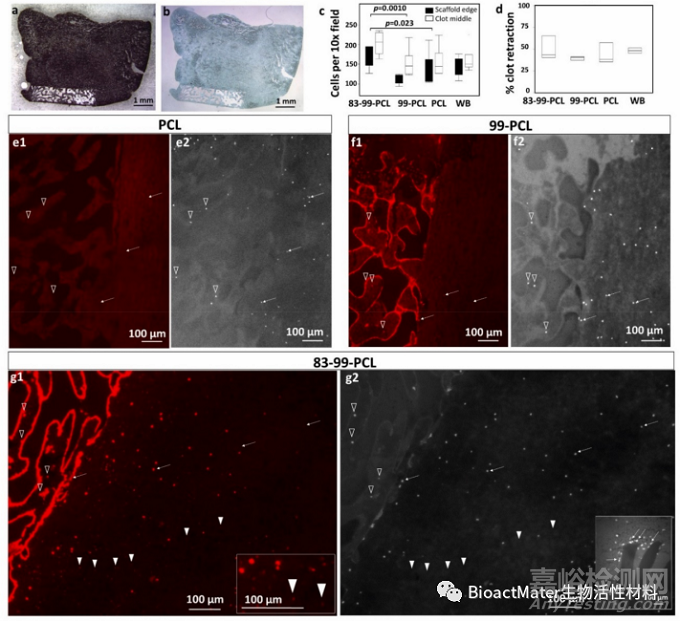
Fig. 2. In vitro blood clot-scaffold interactions after 1 h of in vitro culture at 37◦C. Rabbit blood clot/scaffold cryosections (a) unstained or (b) SafraninO/Fast greenstained, (c) clot cell density (n = 6) and (d) % clot retraction (n = 3). Epifluorescent images of clot samples showing RITC-chitosan (red) and Hoechst 33258-stained cell nuclei (grey scale), for (e) PCL/clot, (f) 99-PCL/clot and (g) 83-99-PCL/clot with chitosan microparticles (arrowheads, g1 inset), clot cells (arrows, open arrowheads), and cell clusters at the edge (g2, inset). Symbols: open triangles: clot cells inside the pores, white arrows: clot cells near the scaffold edge, white arrowheads: 83% DDA chitosan microparticles. Scale bars: (a,b) 1 mm, (c,d) 200μm, (e,f,g) 100μm.
宏观表现:
在将支架植入出血滑车微钻孔后,软骨下血液以与缺陷出血强度(轻、中、重)平行的不同速率渗入 PCL 孔,与壳聚糖涂层无关(图3)。在术后第 1 天,与支架相比,骨软骨缺损术中出血、血肿形成和术后短暂的膝关节积液对6周修复组织的宏观外观影响较小(图3a-d)。修复 6 周后,对照组被白色修复组织覆盖,该组织也覆盖了大部分 99-PCL 支架。许多单纯PCL 和 83-99-PCL 植入物具有暴露的支架(空心箭头,图 3f-h)。83-99-PCL 修复组织呈红色,提示血管生成(粗黑箭头,图 3h)。股骨远端外缘偶尔可见骨赘。所有膝关节滑液清澈,无积液迹象,外周血细胞计数正常。愈合6周后,兔子活动正常,膝盖没有感染迹象。
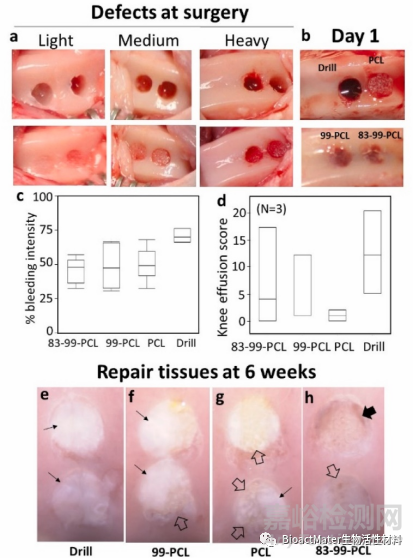
Fig. 3. Osteochondral defect intra-operative bleeding, hematoma formation and transient post-operative knee effusion had minor effects compared to scaffold on macroscopic appearance of 6 week repair tissues. Panels show variable bleeding in drill holes (a-b) before and after implanting the scaffolds, (c) hematoma formation at day 1, and (d) cumulative post-operative knee effusion scores and representative macroscopic appearance of repair tissues for (e) 83-99-PCL, (d) 99-PCL, (g) PCL, (h) drill-only. Symbols (e-h) Thick black arrow: angiogenic tissue; open arrows: exposed PCL bioplastic, thin arrows: cartilage repair tissue.
组织学及影像学表现:
植入体内一天后,PCL支架孔表面检测到壳聚糖涂层,而83%DDA壳聚糖微粒被置换到孔中支架凝块的顶部,这表明来自关节腔方向的软骨下出血的压力将颗粒向上推到骨板区域(图4红色信号)。在 83-99PCL、99-PCL和PCL 支架下方钻孔的弯曲底部形成血肿(图4c,f,图5)。在该区域,细胞在 83-99-PCL下方被耗尽,只在支架边缘发现(图4c黑色箭头)。骨折血肿细胞更均匀地分布在 99-PCL、PCL和单纯钻孔缺陷的下方(图4f)。在83-99-PCL 和99-PCL 支架内和周围观察到含有荧光RITC-壳聚糖的吞噬细胞(图4a,d白色箭头)。这些数据进一步支持了这样的假设,即83-99-PCL 支架对血肿吞噬细胞具有趋化性,并且吞噬细胞可以摄取两种壳聚糖涂层。
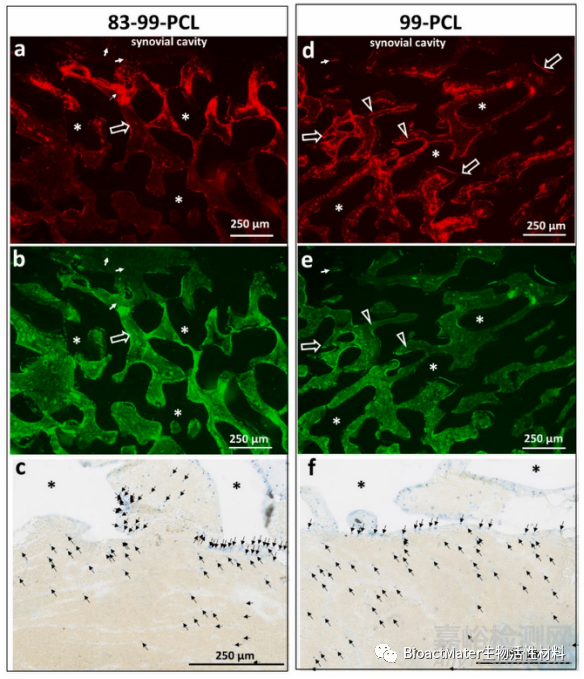
Fig. 4. Hematoma phagocytes swarmed to (a-c) 83-99-PCL and not (d-f) 99-PCL scaffolds after 1 day in vivo. The red signal shows (a) 83% DDA or (d) 99% DDA chitosan and (b, e) matching nonspecific green epifluorescence of the hematoma of the same field. Panels (c & f) show Toluidine blue/ von Kossa stained hematoma below the scaffolds (PCL polymer is indicated by (*) where hematoma cells (blue stain) were displaced towards (c) 83-99PCL and not (f) 99-PCL. Symbols: (a,b,d,e) open arrows: chitosan coating; * = PCL polymer; open arrowheads: detached chitosan coating; thin white arrows: phagocytes with internalized RITCchitosan; (c,f) black arrows: hematoma cells. Scale bars: 250μm.
术后6周,纯钻头缺损显示出持续的经典自发性软骨内修复反应,其中钙化软骨的核心正经历着来自周围骨小梁的强烈的血管性骨入侵(图5,6a-b)。当分析平均横截面积时,单纯缺损在缺损边缘和中部附近时软骨下钙化软骨较多(图7a)。发现主要是软骨组织从骨板的孔隙中浸润出来,并不同程度地覆盖在PCL和99-PCL支架上(图5和6)。这些修复组织的形态表明,软骨是由紧邻骨小孔的间充质干细胞生长形成的。与PCL相比,软骨下软骨平均渗入99-PCL孔隙更远(图5和6c-d & 7a)。83-99PCL支架孔隙以及支架中间明显没有软骨,边缘有0.2 mm2的软骨下软骨(图5和6f-g & 7a)。
观察到83-99-PCL有强烈的血管生成反应,血管围绕着整个支架的孔隙并完全浸润其中(图5o、5和6g红色组织)。单纯缺损和83-99-PCL缺损的血管长度密度(Lv)相似(图7b),然而单纯缺损的血管被矿化组织包裹(图6b),而83-99-PCL的血管则被非矿化纤维组织或未分化的间质包裹(图6g1,g2)。与PCL或99-PCL相比,单纯缺损修复组织和83-99-PCL孔隙组织所含的血管Lv明显升高(图7b)。综上所述,亲炎症的83%DDA壳聚糖刺激了整个PCL支架孔的血管生成,并抑制了软骨生成和成骨。
SafraninO(SafO)染色的软骨修复组织重现缺陷与作为解释变量的软骨下面积呈正相关(R2=0.44,P<0.0001)。在这项研究中,单纯缺损在修复6周后显示出良好的SafO染色的软骨再生(图5、6a和7c)。覆盖支架的软骨修复组织较少,83-99-PCL上的软骨最少,PCL中间的软骨较少(图7c)。99%DDA壳聚糖的主要影响是,在支架中间上方的SafO+软骨复位与单独的PCL相比,保持3倍以上的SafO+软骨复位(图7c)。这种效果部分是由于纯PCL支架中间的软组织重铺不理想(图7d)。
根据对钻孔中矿化组织再生的显微CT测量(图8),初始缺损的骨量分数在单纯缺损修复6周后显著增加,用PCL或99-PCL的缺损略高,而83-99-PCL则较低(图8f)。最初的缺损钻孔横截面积为7.5 mm2,在单纯缺损中,顶部缩小到3.5 mm2,在0.5 mm深的骨小梁处缩小到1 mm2(图8g)。在6周修复的PCL和99-PCL缺损中,残留的钻孔面积略微缩小至6.5 mm2,与第1天的缺损没有明显区别。相比之下,83-99-PCL缺损的钻孔横截面积净增1毫米(图8g)。在6个支架中的4个中,编织的骨质渗入99-PCL和PCL孔隙深处0.3-1毫米。在所有的支架孔隙表面(99-PCL、PCL和83-99-PCL)都检测到骨髓来源的细胞附着。因此,壳聚糖涂层对于细胞在体内粘附到疏水性PCL孔隙表面是不必要的。
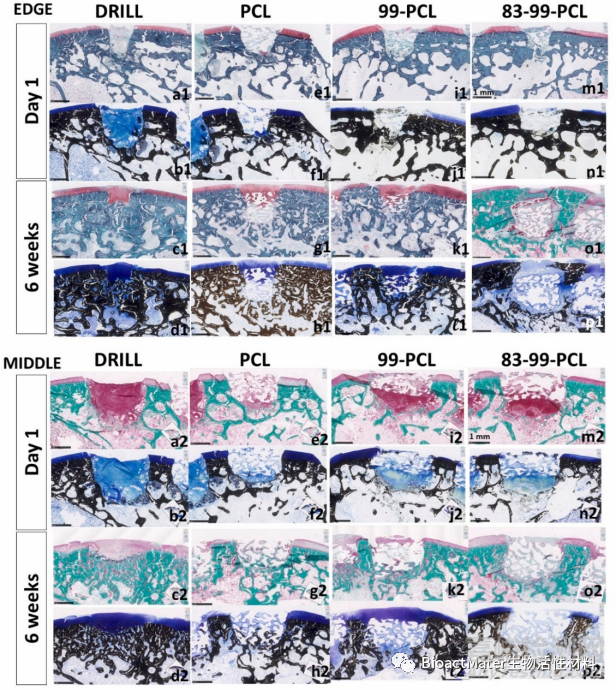
Fig. 5. Nondecalcified histology at the defect edge or middle showing a hematoma filling PCL pores at Day 1 and bone marrowderived repair tissues filling the pores at 6 weeks post-operative. Panels show (a-d) Drill-only, (e-h) PCL, (i-l) 99-PCL, (m-p) 8399-PCL non-decalcified plastic sections, stained with SafO-fast green (Edge: a1,c1, e1,g1,i1,k1,m1), von Kossa/Toluidine blue (edge and middle: b,d,f,h,j,l,n,p) or Goldner Trichrome (Edge: o1; Middle: a2,c2,e2, g2,i2,k2,m2,o2). SafO stains cartilage tissue red, Goldner Trichrome stains bone green and newly deposited bone, blood vessels and cartilage pink/red, von Kossa/Toluidine blue stains mineralized cartilage and bone black, cartilage tissue purple. Scale bar: 1 mm.
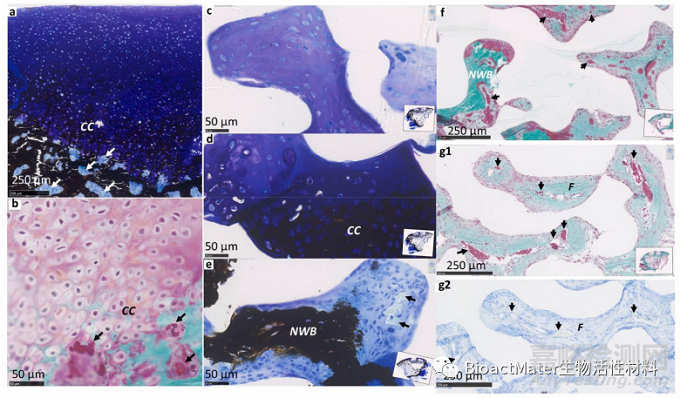
Fig. 6. High-magnification histology of representative 6 week subchondral repair tissues stained with Toluidine blue-von Kossa (a,c,d,e,g2) or Goldner trichrome (b, f,g1). Drill-only defects (a-b) were undergoing endochondral ossification where bone and blood vessels invade calcifying cartilage. Scaffold pore tissues, here shown for 99-PCL, included (c) cartilage, (d) calcifying cartilage (CC), and (e-f) vascular new woven bone (NWB) or unmineralized angiogenic tissue. Angiogenic blood vessels in 83–99-PCL were often enveloped in fibrous tissue (F, in panels g1-g2). Symbols: Arrows: blood vessels. CC: calcified cartilage; NWB: new woven bone. F: fibrous tissue. Scale bars: (a,f,g1,g2) 250μm, (b,c,d,e) 50μm.
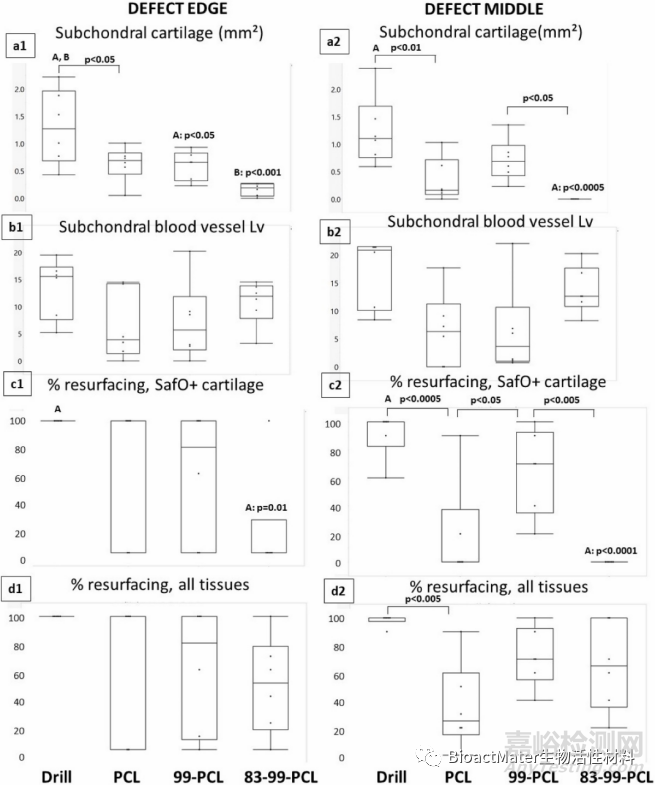
Fig. 7. Histomorphometry of subchondral (a1-a2) cartilage infiltration, (b1-b2) blood vessel stereology of angiogenesis (vessels/mm2), and % defect resurfacing with (c1-c2) Safranin O+ cartilage or (d1-d2) all soft repair tissue from transverse sections near the defect edge (a1-d1) and middle (a2-d2). Graphs show individual data points (dots), median (horizontal line), interquartile range (box) and min-max (whiskers), N = 6.
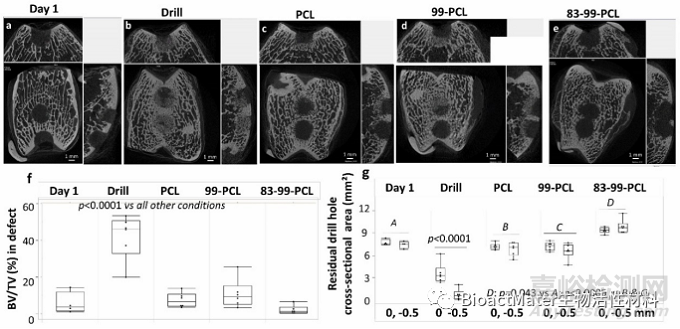
Fig. 8. Example micro-CT images of mineralized tissue formation in microdrill defects at day 1 (a) and 6 weeks (b-e, conditions as indicated), (f) measures of bone volume fraction (%) in a 3 mm diameter 2 mm deep volume of interest, and (g) residual drill hole area (mm2) at the drill hole top and−0.5 mm below the chondralosseous junction (labeled as 0, -0.5 mm, panel g). Graphs show individual data points (dots), median (horizontal line), interquartile range (box) and min-max (whiskers), N = 6. Scale bar: 1 mm.
本研究受到少量生物复制、钻孔中植入物位置相对于软骨-骨连接处的微小差异以及6周终点持续修复的限制。关节运动产生的机械剪切力对支架表面重修具有可变且不受控制的影响,并且在解剖学上弯曲成滑车槽形状的支架形状可能改善了支架上的软骨修复(图9)。
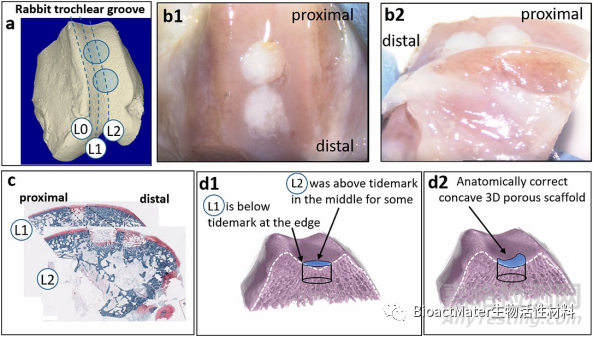
Fig. 9. Diminished resurfacing over some proximal defects was potentially due the curvature of the trochlea and thinner cartilage that led to greater shear forces in the middle of the scaffold, as illustrated through (a) 3-D micro-CT of a rabbit distal femur and sagittal histology sections collected in this study, (b1-b2) macroscopic images of repaired drill holes, (c) serial sagittal sections, and (d1-d2) transverse view of the trochlear groove. Trochlear cartilage is thinner in the proximal area than the distal area, suggesting that shear forces on the flat scaffold that occasionally reached above the tidemark may have been greater in the proximal sites and rubbed off some early mesenchymal tissues growing out and over the pores. A concave scaffold design (d2) would better accommodate shear forces. L0: outside the defect area. L1: edge sagittal section. L2: middle sagittal section.
综上所述,孔径为155μm的 PCL 支架可引发自发的无血管间充质和软骨生成,或在支架深度达1mm的血管生成间充质和成骨。99%DDA壳聚糖涂层促进了软骨下软骨形成和透明样软骨的表面重建。作者还发现软骨是由骨板在植入物上再生(骨源性软骨诱导)形成的,软骨组织可以从通过毛孔和关节支架表面迁移的骨髓组织进行。本实验中观察到血管编织骨和钙化软骨组织浸润支架孔,是对先前测试的用于软骨修复的无细胞BTE支架的改进。
来源:BioactMater生物活性材料